
PG7. Can We Limit Human Population Growth?
Chapter 7
CAIRO — Years ago, when the water buffalo gave plenty of milk and the pigeons and chickens were paraded nightly to the dinner table, Om Mahmoud was healthy and happy with the annual ritual of giving birth to a new baby: another pair of hands in the lush farm fields of the Nile Delta.
But the babies kept dying, one by one. Om Mahmoud would have a new baby, and last year’s infant would die. In all, she went to the birthing table 15 times. Seven lived. And finally, against her husband’s inclinations, she went to a family planning clinic and had an IUD inserted.
“He wanted more children, but I did not, because of my health. He used to think that it would be interfering in God’s ways. But he is ill, and all the responsibility for the income is on me. I insisted, and he was convinced,” recall the 47-year-old woman who supports her husband and children by sweeping stairways in Cairo for about $50 a month.
Now, Om Mahmoud insists her four daughters go to school as her father never allowed her to do.
“When a girl gets an education, she can read, she can learn about programs the government is providing, and from there she can make a decision,” she says.
In the fall of 1994 an important international conference on human population growth was held in Cairo, Egypt. Kim Murphy began her report about that conference as follows:
“The story of Om Mahmoud illustrates the personal nature that is at the base of any discussion on population control. It also encapsulates some of the changes that are underway, which affect population growth in the developing countries. Whatever governments decide, whatever expert opinion may suggest, the ultimate decision concerning population growth rests in the hands of individual men and women. Because of the personal nature of reproduction and its deep cultural and religious connections the subject is a delicate one….”
I. Why Is It Important to Control Human Population Growth?
The environmental consequences of human population growth discussed in Chapter 5 are reasons enough to control it. The danger of doing nothing is to run the risk of producing a human population that overshoots the carrying capacity of the Earth. Population studies have shown that overshooting the carrying capacity usually ends in a population crash—a massive die back due to starvation and disease. That is a situation that population experts believe has already happened in places like Ethiopia, Somalia, Bangladesh, and China, and fear will happen with greater and greater frequency in coming years. However, the most important thing that separates humans from the rest of the animal world is the ability to think ahead. We should be able to deal with our overpopulation problems in better fashion than allowing “nature to take its course.”
II. How Can We Control Human Population Growth?
There are two broad ways that the growth of human population can be slowed:
- Reduction in the birth rate, sometimes called family planning.
- Improvement in the standard of living in the less developed nations where population is growing the fastest. This assumes that as the conditions of life improve the birth rate goes down, a phenomenon already observed by demographers.
Family Planning – Some people think of family planning as a synonym for deliberate termination of pregnancy on demand. The ethics of deliberate termination of pregnancy is complicated enough without this confusion. Family planning refers to a variety of actions and services: giving information to help couples avoid or achieve conception, counseling, educational services, improvement of the health of women and children, and the well being of families. Deliberate ending of pregnancy is just one of the many options considered in family planning discussions.
Strictly speaking the focus of family planning is not on population growth reduction. Rather its goal is to help couples have children when they want them.
Contraception and Religion
Article by Kathleen O’Grady from The Encyclopedia of Women and World Religion (Serinity Young et al. (eds). Macmillan, 1999).
Contraception has been known to humankind from the earliest times. Ancient Jewish sources, early Islamic medical texts, and Hindu sacred scriptures all indicate that herbal contraceptives could induce temporary sterility. Today, however, there exists no uniform position on contraception within each of the major religious traditions; rather, the issue is marked by a plurality of views from followers, religious leaders and scholars. All of the traditions discussed below are founded on notions of fertility and procreation within the family and thus, while the views on contraception vary widely, no religion advocates the goal of a childless marriage or the use of contraception outside of the marriage contract.
The Hebrew Bible promotes prolific childbirth – “be fruitful and multiply” (Gen 1:28) has been taken by both Jews and Christians as God’s “first commandment” – yet there is only one explicit reference to birth control; Genesis 38:9-10, states that during intercourse Onan “spilled his seed on the ground” (coitus interruptus). This was “evil in the sight of the Lord” and was punished by Onan’s death. Jewish Talmudic literature builds on this passage and prohibits the use of any contraceptive device for use by men which would waste the “male seed”; female contraceptives may be permitted for health reasons (danger to the mother or to the potential child). This remains the Orthodox position on contraception, which accepts abstinence as the only permissible birth control method except where health
Conservative and Reform views, which note that sexual pleasure between married couples is permissible and sanctioned by the rabbinical literature, authorize social, environmental and economic reasons for the use of birth control in addition to the health factors accepted by Orthodox practice, and leave the decision to individual choice (declared formally at the Central Conference of American Rabbis, 1930; and the Rabbinical Assembly of America, 1935).
Prior to the 1930s all Christian denominations were united in their firm rejection of contraceptives. The Lambeth Conference of the Church of England (1930) marks the first departure from this unanimous prohibition, by advocating the use of artificial contraception when abstinence was deemed impracticable. The Federal Council of Churches (1931) equally adopted a policy of conservative advocation for artificial birth control methods. Most major Protestant traditions followed suit, and by 1961, the National Council of Churches declared a liberal policy on contraceptive use, subject to mutual consent between couples.
The total prohibition of artificial birth control methods by the Roman Catholic church, declared by Pope Pius XI in his 1930 encyclical, Casi Connubii, was maintained by the 1968 Humanae vitae (the encyclical of Pope Paul VI), and constitutes the present day policy of the church. The Catholic position on contraception is highly influenced by the natural law theory of Aristotle, Augustine and Aquinas, which deems that sexuality has as its end purpose, procreation; to interfere in this end would be a violation of the natural law, and thus, a sin. This view is maintained by some Anglicans, Evangelicals, and Christian fundamentalist denominations as well. The Catholic Church sanctions only abstinence and the Natural Family Planning method (NFP) as suitable techniques for birth control.
Unlike the Catholic tradition, the Eastern Orthodox Church does not discern a moral difference between artificial or natural birth control methods. They note that many Church Fathers, as well as the Pauline texts in the New Testament, do not strictly limit sexual intercourse to procreation; the Orthodox position is that sexual intercourse also constitutes an expression of love within the marriage contract. No official statement has been made on prohibitions for artificial contraceptives, while deliberate ending of pregnancy, infanticide and permanent sterilization have been condemned. The Orthodox Church allows a married couple to make their own decisions on contraceptive use.
There is a widespread variation on attitudes to contraception in the Islamic faith. The Quaran states: “You should not kill your children for fear of want” (17:31; and 6:151). Critics of birth control argue that this can be extended to include a ban on all family planning methods, while advocates of birth control indicate that this passage explicitly refers to infanticide, and note that there is no prohibition against birth control in the Quaran.
Further, the Hadith and Sunna literature clearly permits the practice of coitus interruptus (‘azl), and sources indicate that ‘azl was practiced by the prophet Muhammed himself (Sunna related by Jabir). Those in favour of contraception argue that artificial birth control is morally the same as ‘azl and therefore to be accepted. Most Muslim traditions permit the use of birth control where health reasons are an issue or where the well-being of the family is concerned; this affords great flexibility and latitude in interpretation and is reflected by the vast differences in policies on family planning by distinct Muslim groups and countries. Despite varying viewpoints, the emphasis remains on procreation within the family as a religious duty. There is unanimous rejection of sterilization and deliberate termination of pregnancy.
Hinduism actively encourages a prolific procreation within marriage but there is no prohibition against birth control in the Hindu religion. The Upanishads describe a birth control method (Brihadaranyaka Upanishad) and temporary abstinence is advocated in the Shastras, while deliberate ending of pregnancy is condemned.
Still there is a wide variance of views on contraception by Hindu scholars: Gandhi advocated birth control based on abstinence and not through artificial means, while Radhakrishnan and Tagore, on the other hand, promoted the use of artificial methods. India was the first nation to establish a governmental population strategy based on birth control measures.
Common concerns unite all major religious traditions on the issue of birth control. The critics of family planning in each tradition fear that contraceptive use will encourage immorality and illicit sex, while further, many non-Western faiths fear that liberal contraceptive policies encourage a Western model of living that would destroy the family and family values. Feminist commentators have viewed prohibitions on birth control as a means to control female sexuality and independence.
All other methods offer various degrees of protection against an unwanted pregnancy. In many countries information about the birth-control pill, condoms, diaphragms, and spermicidal jellies, is widespread and the products themselves are increasingly available. These methods of birth control are generally acceptable to most members of the Protestant and Jewish communities. Wherever educational programs concerning the facts of the human reproductive cycle and the methods of avoiding conception have been introduced, the birth rate has been reduced.
Most religious groups in the U.S. report contributing in some form to international humanitarian assistance. Others do not. Some offer financial support for family planning programs. The difference is probably due to the continuing conflict surrounding the issue of deliberate termination of pregnancy and its association with family planning.
Efforts at population control easily stir up controversy. What has been learned is that population policy that works must not violate a culture’s integrity.
III. Avoiding Conception as a Means of Population Control
According to information from a Population Council Report dated February, 1994, approximately one in four births in the developing world (excluding China) is unwanted, and even more are unplanned. Unplanned births are often detrimental to the development of the child, not to mention the disruption caused in the life of the mother and to family relationships.

PG7.1. Investigation:
Population Control—Cultural Connections
Much of the debate centered around the termination of any pregnancy is whether or not a human being with full human rights is being deliberately killed, which to a large segment of our population, constitutes murder.
Part A
Go to the web site https://en.wikipedia.org/wiki/Human_embryonic_development to look at stages in human embryonic development. Can you determine for yourself when the embryo should be considered human? Discuss this with your classmates and write your opinion, backing it up with your observations. To help you do this, you could examine pictures of human embryos at different stages. Grays Anatomy is a book which has excellent diagrams of each stage. You could look at the video called The Miracle of Life or do a video search for “stages in human embryonic development”.
To avoid terminating a pregnancy, many feel that the problem should be solved even before the egg and sperm get a chance to meet.
There are several ways to prevent the sperm and egg from coming together. These methods of contraception fall into the following categories:
• Not engaging in sexual activity – abstinence
• Preventing a follicle from developing – birth control pills
• Placing a barrier between sperm and egg—condoms (male/female), cervical caps, diaphragms
• Killing the sperm – spermicides
• Surgery – blocking the sperm or egg with surgical procedures like tubal ligations (in women) or vasectomies (in men)
• Timing – avoiding intercourse during the period of maximum fertility
How well do these methods of birth control work? You will note from the table on the next page that only one is foolproof. Total abstinence from sexual relations is the only guaranteed method of birth control. It is also the only method agreed upon by all cultures in all places, with one stunning exception! The abstinence in many cultures applies only to females, and NOT to males. Some cultures will go to extremes to keep their young women virginal, while young men are expected to “sow their wild oats”.
Part B
Do research on Internet to find out which methods of birth control are considered acceptable or feasible in various cultures. Each student or group could take one or two methods and research reasons why it is or is not used. Look at education, cost, and status of women.
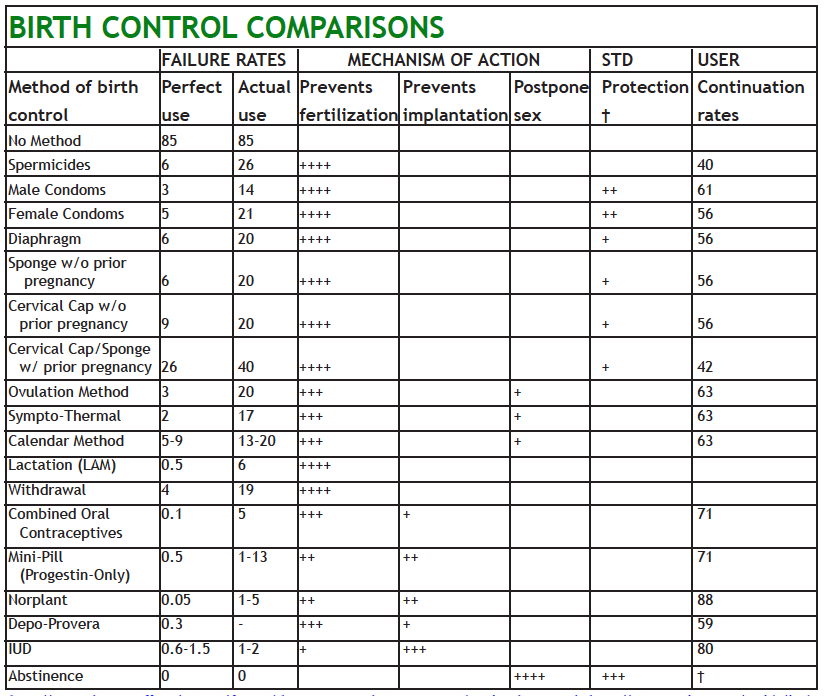
This chart compares reversible contraceptives. Each method is listed with its estimated “perfect use failure rate,” that is, the percentage of pregnancies which occur if the method is used perfectly and consistently. The “actual failure rate,” also listed below, is the percentage of pregnancies reported by typical users. All of these figures are among couples using the specified method for one year. The columns in the center indicate how each method works, giving an idea of which mechanisms are employed as birth control. Failure rates for hormonal methods and the IUD tend to be lower because of interceptive mechanisms which take effect when fertilization is not prevented. On the right are indications as to sexually transmitted disease (STD) protection and one year continuation rates for each method.
IV. Deliberate Ending of a Pregnancy as a Means of Population Control
Deliberate ending of pregnancy has always been a controversial subject of discussion among those who surround us. It is nearly impossible to find someone who does not have an opinion about deliberate termination of pregnancy. Since both sides have strong arguments in defense of their viewpoints, debates on the topic usually go nowhere. An unwanted child is a pitiful thing, but the thought of terminating something that if left to run its natural course would result in a birth of a human being gives many people a feeling of abhorrence. However, it is the government’s responsibility to ensure the well being of all its citizens, and the well being of all individuals includes the personal control of one’s own body.
According to the law a woman could legally have deliberate end of pregnancy up to a set number of weeks into a pregnancy only—after that a deliberate ending of pregnancy would be illegal. The applicable laws in the United States emanate from two basic governmental sources: (1) the legislatures of the several states and territories and (2) the United States (i.e., the “federal”) Supreme Court. The state legislatures, being responsible for the production of most criminal laws, are the traditional source of regulation of the termination of pregnancy. Thus, from the decline of common law (judicially created) crimes in the early 19th century, to the intervention of the United States (federal) Supreme Court in the 1970s, state legislatures widely criminalized deliberate termination of pregnancy. In 1973, in the case of Roe vs. Wade, the United States Supreme Court ruled that the 14th Amendment to the United States Constitution provided a fundamental right for a woman to end pregnancy. The Supreme Court held that the “right to privacy,” established by the Court’s precedents in the contraception cases of the 1960s and early 70s, assured the freedom of a person to end pregnancy unless the state had a “compelling interest” in preventing such an action. The Court then held that, though the state had an interest in protecting fetal life, this interest did not become adequate to allow banning the deliberate termination of any pregnancy until fetal viability occurred in the third trimester of pregnancy. All the state laws that regulated deliberate ending of pregnancy during the first six months of pregnancy, except for the purpose of protecting maternal health during the second trimester, were invalidated.
Additional Laws Restricting the Deliberate Termination of a Pregnancy
16 states still have pre-1973 laws on the books restricting deliberate termination of pregnancy even though they are clearly unconstitutional and nullified under Roe vs. Wade.
There have been many attempts since 1973 to reduce free access to deliberate ending of pregnancy. Laws have been passed by some states and at the federal level to:
- require counseling and/or a cooling-off period before a deliberate ending of pregnancy,
- require an underage woman to obtain permission from a parent, guardian or court
- end financial support for women in poverty who seek to deliberately terminate pregnancies,
- ban deliberate termination of pregnancy after viability of the fetus unless required to preserve the woman’s life or health.
The U.S. Supreme Court ruled in its famous 1973 Roe vs. Wade decision that:
- a woman and her doctor may freely decide to terminate a pregnancy during the first trimester,
- state governments can restrict access to the medical help in deliberate termination of pregnancy after the first trimester with laws intended to protect the woman’s health,
- if the woman’s health or life are at risk, medical help in deliberate ending of pregnancy after fetal viability must be available; state governments can prohibit other deliberate terminations of pregnancies.
Today most people who favor deliberate ending of pregnancy focus on a woman’s rights and the people opposed to deliberate ending of pregnancy focus on a fetus’ rights. Both agree that the life of a child is a precious thing that deserves the full protection of the law. There would even be nearly universal agreement that it is a woman’s exclusive right to make decisions concerning her body.
The crucial question of the controversy is, “When does a fetus become a human being?” Unfortunately science cannot give a clear answer to this question and conservative religious opposition has increased since the early 1980s.
Deliberate ending of pregnancy is at present the most widely practiced form of family planning in the world. According to the World Health Organization an estimated 50 million women each year resort to deliberate ending of pregnancy to prevent unwanted births. The fact that it has a long history and that many women do it does not, in the view of the opponents, make it morally right. Many of them hold that the life of a human being starts with the union of a sperm with an egg and that the growing fetus should be treated as a human being. From that point of view destruction of a fetus is the same as murder of an individual.
The courts and most people in the U.S. have adhered to a different view. The nine months of pregnancy are divided into thirds. During the first three months (first trimester) medical access to deliberate termination of pregnancy is guaranteed by law. It is a decision and responsibility of the woman.
The opposition of the Roman Catholic Church to any interference with conception except for the avoidance of sex during a woman’s fertile period is well known. At one time Thomas Aquinas had held that the fetus went through various stages of development before it acquired a human spirit, which did not happen until about 45 days after conception. This became the Church’s position until 1869 when church law changed. Today, Church authorities admit that they do not know when a fetus becomes a person but that doubt is sufficient reason to oppose all deliberate termination of pregnancy.
PG7.2. Investigation: Difficult Questions
Is finding a successful method of birth control the only problem? What if a method is found that an individual would find effective, but it is forbidden for use by their government? How much can a government interfere with the lives of individuals?
Consider these difficult questions:
- How much should the government of a free nation have to say about birth control?
- Should it be regulated?
- If so, to what extent?
Work with a group of students to come up with answers to these questions. When you can agree, report on your opinions to the class and be prepared to back them up. If you cannot agree, allow for a minority opinion, making sure that both sides have reasoned arguments for their opinion.
V. Education and Emancipation of Women
All over Western Europe after World War II and in other industrialized countries, women began to leave the house for the world of outside work, and went to school for career education. As women moved out of the home into offices and factories increased education gave them the tools to do jobs other than child raising and housekeeping and it gave them a different image of themselves. Expanded life choices were available. Using birth control, women could choose when they wished to start a family. Statistics showed that invariably the more educated a woman was, the later she tended to marry and the fewer children she had.

{kind=link}
In many of the less developed countries, however, the role of women has not changed. Young girls are forced by social pressures, coercion and sometimes even violence into early marriages and frequent childbearing. Where boys are valued more highly than girls, wives are expected to keep having children until the desired number of sons are produced. Where women are denied education, independence, property ownership, legal and social rights they will continue to rely on childbearing as a source of status and security.
Multiple births can take a terrible toll on the mother. Every pregnancy is a drain on her health. This is especially true in situations where the woman not only works in the fields but where low living standards do not give her the support she needs. In many cultures where women work the fields and prepare the food, they usually eat last and only the leftovers. In these places women are limited to roles as field workers, preparation of meals, home keepers and child bearers. Without rights and education, they do not have the economic or political strength to change their roles.
As we have seen, where women have some degree of control over their own destinies, the birth rate declines and female health improves. Where education of women is encouraged the size of families is much smaller. One of the methods to reduce population growth then, is to improve their situation.
VI. Women’s Rights

Photo by USAID via Wikimedia Commons
The controversy that surrounds deliberate ending of pregnancy impinges on the right of a woman to control her own life. Those who support deliberate ending of pregnancy as a legitimate choice point to the consequences of forcing unwilling parenthood on women. Childbearing permanently disrupts the course of life. It curtails education, employment opportunities, and changes the social status of women. Where a child is unwanted or where there is a lack of ability of the parents to support it, the effect on the child’s development can be disastrous.
Going beyond the question of the right of women to make their own choice with regard to deliberate ending of pregnancy, the right of women to birth control measures is still an issue in some cultures. Many people see access to effective birth control as a personal liberation that gives a woman the means to shape her own destiny and stabilize her family’s life. For some men this is a perceived threat to their authority. Others may see birth control as a means toward an immoral life or as giving a woman too much control.
VII. Reducing the Birthrate by Economic and Social Change
Birth rates are influenced by many factors. The family planning movement is one of them. Population experts point out that economic and social changes also influence birth rates. The theory of the demographic transition was developed out of the experience of the industrialized countries of the West. Many experts expected developing countries in the rest of the world to follow the same pattern. The expectation was that, as industrialization proceeded, a reduction in the birth rate would follow economic improvement. The slogan of the World Population Conference in 1974 was “development is the best contraceptive.” In the last century in the U.S. and the U.K. this process took many decades. However, recent studies have shown that a reproductive change is already under way in the developing world.
All over the developing world women from different cultures, and from different social and economic backgrounds have started to desire smaller families. Birth rates have begun to fall even in the absence of improved living conditions. They have declined by about a third in the last thirty years. Where women formerly had an average of six children they now have four. These changes have taken place in countries as different as Thailand, Colombia, Morocco and Turkey.
Although many factors must necessarily be present to bring about declining birth rates, among them is the distinguishing characteristic of the modern age — information exchange. It is no longer noteworthy that a television antenna may sprout from the roof of the poorest home. Remote villages that may not have a school have a communal television set around which many members of the community gather in the evening. It is impossible to measure what changes in attitudes and values are taking place as viewers watch messages about personal and family health and see portrayals of different, and sometimes foreign, life-styles. However, in some countries popular entertainment shows also encourage family planning. They seem to have had great effect. Other methods of communication, like radio and visits of traveling nurses, are also being used to spread information concerning family planning.
If contact with the wider world has changed attitudes concerning family life, the availability of contraceptive methods have provided the means to put new ideas into action. In the developing countries 38 percent of women in their childbearing years now use contraceptives. There is increasing use of condoms as a contraceptive technique as well as protection from sexually transmitted diseases and AIDS. Voluntary sterilization is increasingly common in Latin America and in India. Birth rates have declined even in the sub-Saharan lands of Botswana, Kenya and Zimbabwe.
In Kenya, for example, where the culture previously favored large families the growing shortage of agricultural land changed the aim of family life. Strong programs by the Kenyan government and volunteer population organizations provided information and contraceptives throughout the country. Better education for women increased their status and promoted the use of contraceptives. The result was that between 1984 and 1989 contraceptive use rose 59 percent.
One of the social benefits of smaller families is the concentration of family energy and assets on a smaller number of individuals. This result is true of families in the U.S. as well as elsewhere. The Rand Corporation, a study group that researches such questions, reported in 1994 that the largest family factor contributing to higher scores on the National Assessment of Educational Progress tests were a drop in family size.
VIII. The Future of Population Growth
If the worldwide decline in birth rates generates optimism with regard for the long-term future of human population, there is still the sobering thought that, despite the decrease in birth rates, the total human population will continue to grow. The number of people in the world is expected to double to 10 billion by the year 2050.
One of the reasons is that a large part of the world population has not yet reached its reproductive years. In the developing countries more than one third of the population is under 15 years of age. Even if future couples practice family planning and have 2 or fewer children, the number of childbearing couples will result in a population increase.
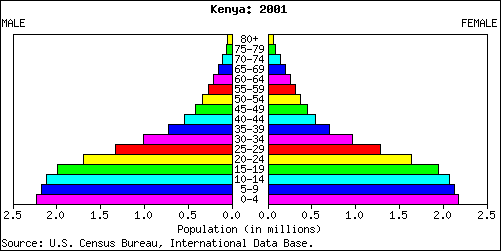
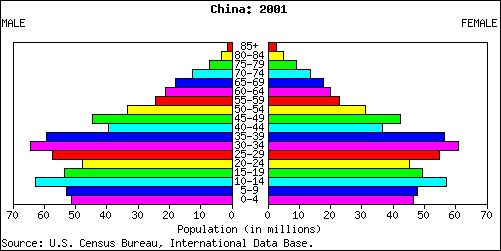
The population age structure graphs shown here compare a rapid growth country (Kenya), a slow growth country (China) and a negative growth country (Russia).
Kenya Population Pyramid
China Population Pyramid
Russia Population Pyramid
Question 8.4.
How do the shapes of the graphs differ?
Question 8.5.
How do the percentages of young children compare in the three countries?
Question 8.6.
What can you predict about the future populations of Kenya and Russia from the information in the graphs?
Question 8.7.
What will happen in 10, 20 and 30 years?
Question 8.8.
Based on the information in the graphs, what can you predict about the needs for each of the countries in the years to come?